Cool video from John Green about why the pre-Obamacare U.S. health care system has been so expensive. Almost everything he talks about is on our reading list. By the end of the semester, you will be able to give this talk! (John does make one or two mistakes that we can fix.)
Most exam questions are 10 points each. To be on track for an A, get 100 points worth done or submitted by Oct. 24. To get an A, get 200 points by the end of the semester.
Redos are permitted until the last class. If it is the last week of class and you don't have 200 points yet, and you want an A, submit an extra question or two, in case you do not get full credit on everything.
The semester point cutoffs for different grades will be
200 or more for an A
175 or more for a B+
150 or more for a B
125 or more for a C+
100 or more for a C
HSPM 714 MPH Section J50
Economics Perspectives on U.S. Health Care
Fall 2013
Samuel L. Baker, Ph.D.
Professor Emeritus
Department of Health Services Policy and Management
Arnold School of Public Health
University of South Carolina
Columbia, SC 29208
E-mail:
I have retired. This subject matter is not being offered in this form. References below to Blackboard no longer work. I will occasionally maintain and update this web site for your reference.
The class meets at 6:00pm-8:45pm on Thursdays in
Swearengen 2A07.
Class meetings are available live over the internet to registered students. The class meetings are recorded as well. Students can view the recordings at their convenience.
Office hours: Thursdays 1:30pm to 4:30pm in the HSPM computer lab.
Goals
HSPM 714 J50 follows the money in the U.S. health care system.
It introduces the application of economic theory to decisions
regarding the amount, organization, and distribution of health care
services in the United States. The goals of the course are:
to provide an economics perspective for management
decision-making
to provide theoretical groundwork for the study of finance,
accounting, marketing, and planning
to enable you as future health care managers to anticipate policy changes and their effects
to enable you as future health care managers to play positive
roles in the reform of health care
Competencies
You will demonstrate on the course's written assignments and through
class participation:
that you understand and can use basic economics concepts, such
as supply, demand, marginal analysis, the theory of capital, and
cost-benefit analysis,
that you can analyze the economic institutions of the United
States health care system,
that you can discuss controversies surrounding the development
of health insurance and the government's role in providing, financing,
and regulating health services.
What you need to have to take
this course
Prerequisite courses: None. No prior study of economics is
required for this course.
Interactive instruction: A group of
interactive instructional tutorials is at https://sambaker.com/econ/.
The interactive tutorials introduce basic economics concepts, and assume no economics background. Your work with the
interactive tutorials is not monitored or graded. These
tutorials
are integrated into the Class Schedule and Readings, as shown below.
All
of the interactive tutorials are available all semester, so you can use
or reuse them at any time.
Course Work for Credit
There will be two take-home exams, due Oct. 24 and Dec. 12.
Each exam counts for one-half of the grade.
The questions will be available well in advance at a link here on this web page.
Class Schedule and Readings
Advice for the overwhelmed: If the reading for this course seems
like a lot, see How
2 Read an Article.
August 22 Introduction to the Course
How the course will
operate, and the general shape of the US health care economic sector.
Stocks
and flowsA basic distinction in economics. It will help you understand the GDP concept. It also helps with understanding monetary policy, such as why the Federal Reserve can push a lot of money out to banks ("print money") during a recession and not spark price inflation.
The Gross Domestic ProductGo through for a general discussion of how this
important economic statistic is conceived.
U.S. National Health Spending in 2011:
Lecture notesI talk you through the most recent numbers for the size and shape of the
U.S. health care system.
What economists mean by markets, supply and demand, elasticity, and risk and risk aversion. These are building block concepts towards assessing having a free market in health care.
Colonoscopy price is the example. You provide the explanation. What is driving this, supply or demand? 8/28/13: Having trouble accessing New York Times web site. May put off discussing this article.
September 5
No class this week.
September 12
Health Insurance
Building-block ideas relating to the economic theory of insurance
Kaiser Family Foundation, The Story of Medicare: A TimelineYouTube introduction to Medicare. Medicare covers the elderly, some disabled, and people with kidney failure.
It is run by the Federal government, with Federal tax money plus some premium payments and copayments by the beneficiaries. http://kff.org/medicare/ is their page with lots of information about Medicare.
Kaiser Family Foundation, Medicaid: A Primer. Medicaid is the Federal-state program that covers lower-income persons in certain categories, mainly children, pregnant women, and disabled people. Obamacare extends Medicaid eligibility to all poor persons. In the states that cooperate, half of the uninsured who become insured will get their insurance through Medicaid.
What things have to be true for the free market to give a good result? Are those things true for health care?
Information and uncertainty in health care choice, implications for letting the free market rule
Blackboard Arrow, K., "Uncertainty and the Welfare Economics of Medical
Care," American Economic Review, December 1963, 53(5),
pp. 941-973. Important. But difficult. Don't get bogged down. The blog posts below by Reinhardt will help, as will my notes below.
If you have time for only one article, read the last one, by Gawande.
Blackboard Wennberg, J.E., McPherson, K., Caper, P., "Will Payment Based on
Diagnosis-Related Groups Control Hospital Costs?" N Engl J Med,
August 2, 1984, 311, pp. 295-300. People
living in different areas get very different care. This article created
a whole area of health services research.
Blackboard Hillman, B.J., Joseph, C.A., Mabry, M.R., Sunshine, J.H.,
Kennedy, S.D., Noether, M., "Frequency and Costs of Diagnostic Imaging
in Office Practice -- A Comparison of Self-Referring and
Radiologist-Referring
Physicians," N Engl J Med, Dec. 6, 1990, 323(23), pp.
1604-1608. A notorious example of the abuse of supply-sensitive care (see the Dartmouth Atlas readings below for what "supply-sensitive care" is)
The Dartmouth Atlas, http://www.dartmouthatlas.org/, has extensive data
and analysis on medical practice variation. They argue that there are three categories of medical care. Here they are, with links to reports:
Effective care, which is clearly indicated for the diagnosis
Preference-sensitive care, for which different patients may evaluate the risks and benefits differently
Supply-sensitive care, determined by the economic benefit to the providers, more than by the needs and preferences of the patients
Atul Gawande, The Cost Conundrum: What a Texas Town Can Teach Us about Health Care, The New Yorker, June 1, 2009. President Obama had all his policy people read this.
The trendy way to control health care spending is to have a big deductible and copayments. (Obamacare does exempt some "preventive" services.)
People do get less health care when
they have to pay more. To use the jargon, the demand for
health care has some elasticity. The elasticity is pretty low,
especially for people seeking care for serious symptoms, but it's not 0.
The articles go on to investigate whether people who buy less care are worse off as a result.
If they are not worse off, then it is wasteful to let people get care without paying out of pocket.
Are all the costs being considered? How good are people at determining what care they can do without?
Blackboard Brook, R.H., et al, "Does Free Care Improve Adults'
Health? Results from a Controlled Trial of Cost Sharing in Health
Insurance," N Engl J Med, December 8, 1983, 309, pp.
1426-1434.
Supplemental:Blackboard Himmelstein, D.U., Woolhandler, S., "Free Care, Cholestyramine,
and Health Policy," N Engl J Med, December 6, 1984, 311,
pp. 1511-1514.
Read quickly for the main ideas.
Blackboard Shapiro, M.F., Ware, J.F., Sherbourne, C.D., "Effects of Cost
Sharing on Seeking Care for Serious and Minor Symptoms," Annals of
Internal Medicine, February 1986, 104, pp. 246-251.
Read quickly for the main ideas.
Blackboard Rasell, M.E., "Cost Sharing in Health Insurance -- A
Reexamination," N Engl J Med, April 27, 1995, 332(17),
pp. 1164-1168.
Malcolm Gladwell, interviewed about "The Moral-Hazard Myth" on
the Al Franken Show (radio), August 25, 2005: A 19-minute mp3. The ideas in the article, with more implications drawn out. For those who like to hear, as well as read.
Gladwell said that the reason we don't have universal health insurance is that our leaders think that we're better off without it. Listen carefully to then-President Bush's "objective" for our health care system, from July 2007. It's in the first 20 seconds of the clip.
Learning objectives: The history and results managed care.
Managed care development
Blackboard Mayer, T.R., and Mayer, G.G., "HMOs: Origins and Development" N
Engl J Med, February 28, 1985, 312, pp. 590-594.
When HMOs were cool
BlackboardWare, J.E., et al, "Comparison of Health Outcomes at a Health
Maintenance Organisation with Those of Fee-for-Service Care," Lancet,
May 3, 1986, pp. 1017-1022.
Blackboard Siu, A.L., Leibowitz, L., Brook, R.H., Goldman, N.S., Lurie, N.,
Newhouse, J.P., "Use of the Hospital in a Randomized Trial of Prepaid
Care," JAMA, March 4, 1988, 259, pp. 1343-1346.
Blackboard Ware, J.E., Bayliss, M.S., Rogers, W.H., Kosinski, M., Tarlov
A.R., "Differences in 4-year Health Outcomes for Elderly and Poor,
Chronically Ill Patients Treated in HMO and Fee-for-Service
Systems: Results from the Medical Outcomes Study," JAMA,
October 2, 1996, 276(13), pp. 1039-1047.
Blackboard Bodenheimer, T.S., and Grumbach, K., "Capitation or
Decapitation," JAMA, October 2, 1996, 276(13), pp.
1025-1031. How the money flows in IPA HMOs
Blackboard Kuttner, R., "Must Good HMOs Go Bad? First of Two Parts: The
Commercialization of Prepaid Group Health Care," N Engl J Med
May 21, 1998, 338(21), pp. 1558-1563.
Blackboard Himmelstein, D.U., Woolhandler, S., Hellander, I., Wolfe, S.M.,
"Quality of Care in Investor-Owned vs Not-for-Profit HMOs," JAMA.
July 14, 1999, 282:159-163
Blackboard Fries, J.F., Koop, E., et al, "Reducing Health Care Costs by
Reducing the Need and Demand for Medical Services," N Engl J Med,
July 29, 1993, 329(5), pp. 321-325. The
authors are renowned public health leaders. This is conventional
wisdom. But is it right?
Blackboard Russell, L.B., "The Role of Prevention in Health Care Reform," N
Engl J Med, July 29, 1993, 329(5), pp. 352-354. Worth
a fairly careful read. What is the basis of Russell's disagreement with
the conventional wisdom?
Blackboard Huntington, J., Connell, F.A., "For Every Dollar Spent -- The
Cost-Savings Argument for Prenatal Care," N Engl J Med, Nov.
10, 1994, 331(19), pp. 1303-1307.
Blackboard Morgan, R.O., Virnig, B.A., DeVito, C.A., Persily, N.A., "The
Medicare-HMO Revolving Door -- The Healthy Go In and the Sick Go Out," N
Engl J Med, July 17, 1997, 337(3), pp. 169-175. Glance through for the main idea, which is that early Medicare HMOs encouraged high-cost patients to leave, until their costs were back to normal.
Blackboard Reinhardt, U.E., "Perspective: Spending More Through 'Cost
Control': Our Obsessive Quest to Gut the Hospital," Health
Affairs, Summer
1996, 15(2), pp. 145-154. You see how a top-notch economist thinks. Relevant for this
week is how the author uses the "incremental cost" (marginal cost)
concept.
Blackboard Brown, M.L., Kessler, L.G., Reuter, F.G., "Is the Supply of
Mammography Machines Outstripping Need and Demand?" Annals of
Internal Medicine, October, 1, 1990, 113(7), pp. 547-552. Excess
capacity did not lead to falling prices for mammogram screenings.
Blackboard Reinhardt, U.E., "Resource Allocation in Health Care: The
Allocation of Lifestyles to Providers," The Milbank Quarterly,
1987, 65(2), pp. 153-176.
DRG payment for hospitals
Blackboard Roe, B.B., "The UCR Boondoggle: A Death Knell for Private
Practice?" N Engl J Med, July 2, 1981, 305(1), pp.
41-45. Before Medicare introduced DRG-based payment, in 1983, fee-for-service was how most doctors and hospitals got paid.
Providers charged for each service rendered, setting prices according to what they thought they could or should get.
By the 1980s, prices had gotten seriously out of whack with costs.
DRG and RBRVS Lecture notesPricing in health care didn't follow the competitive market model, so the Federal government stepped in. Private insurers followed the government's lead.
Blackboard Qian X, Russell LB, Valiyeva E, Miller JE. "'Quicker and sicker' under Medicare's prospective payment system for hospitals: new evidence on an old issue from a national longitudinal survey."
Bulletin of Economic Research, 2011, 63(1):1-27.
Blackboard Simborg, D.W., "DRG Creep: A New Hospital-Acquired Disease," N
Engl J Med, June 25, 1981, 304(26), pp. 1602-1604.
Blackboard Baker, S.L., Kronenfeld, J.J., "Medicaid Prospective Payment:
Case-Mix Increase," Health Care Financing Review, Fall 1990, 12(1),
pp. 63-70.
RBRVS payment for doctors -- A tool for controlling physician fees
Blackboard Hsiao, W.C., Braun, P., Dunn, D., Becker, E.R., DeNicola, M.,
Ketcham, T.R., "Results and Policy Implications of the Resource-Based
Relative-Value Study," N Engl J Med, September 29, 1988, 319(13),
pp. 881-888.
Blackboard Hsiao, W.C., Braun, P., Yntema, D., Becker, E.R., "Estimating
Physicians' Work for a Resource-Based Relative Value Scale," N Engl
J Med, September 29, 1988, 319(13), pp. 835-841.
Where we are with pricing
Blackboard Reinhardt, Uwe E., "The
Pricing Of U.S. Hospital Services: Chaos Behind A Veil
Of Secrecy," Health Affairs,
January/February 2006; 25(1): 57-69.
Blackboard Pattison, R.V., and Katz, H.M., "Investor-Owned and
Not-for-Profit Hospitals: A Comparison Based on California Data," N
Engl J Med, August 11, 1983, 309, pp. 347-353. A classic. For-profit hospitals charged more and collected more.
Blackboard Himmelstein, D.U., Woolhandler, S., "Cost Without Benefit:
Administrative Waste in U.S. Health Care," N Engl J Med,
February 13, 1986, 314, pp. 441-445. Letters and authors'
rejoinder, N Engl J Med, October 16, 1986, 315, pp.
1033-1035.
Supplemental (but cute):Blackboard Grumet, G.W., "Health Care Rationing Through Inconvenience: The
Third Party's Secret Weapon," N Engl J Med, August 31, 1989, 321(9),
pp. 607-611.
Blackboard Woolhandler, S., Himmelstein, D.U., "The Deteriorating
Administrative Efficiency of the U.S. Health Care System," N Engl J
Med, May 2,
1991, 324(18), pp. 1253-1258.
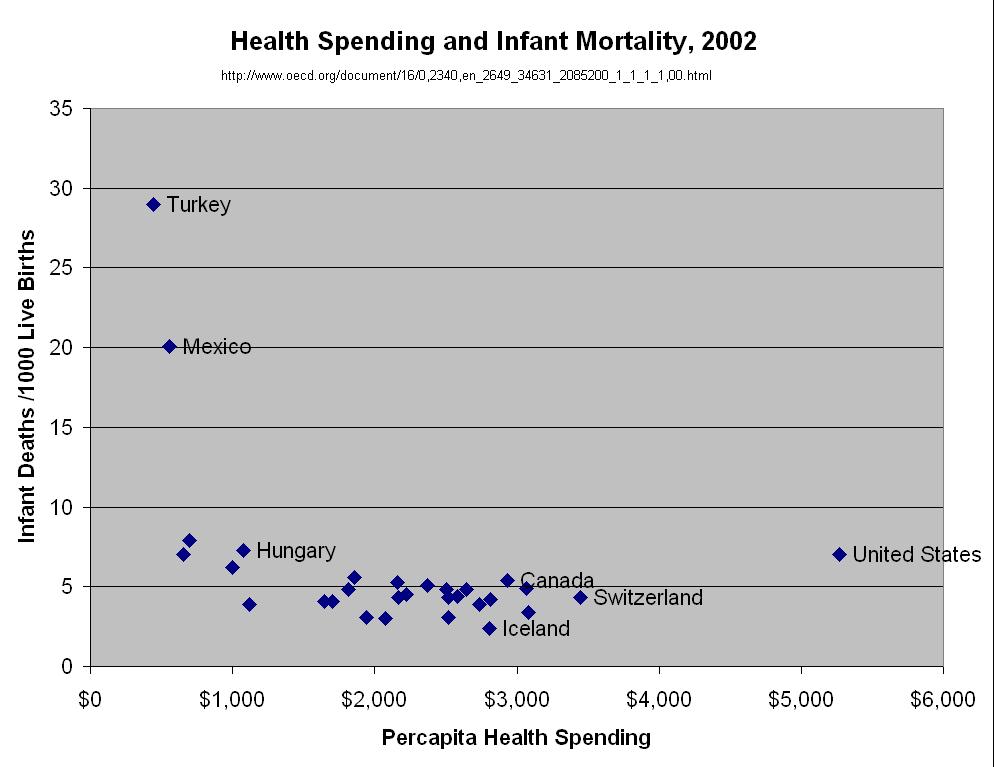
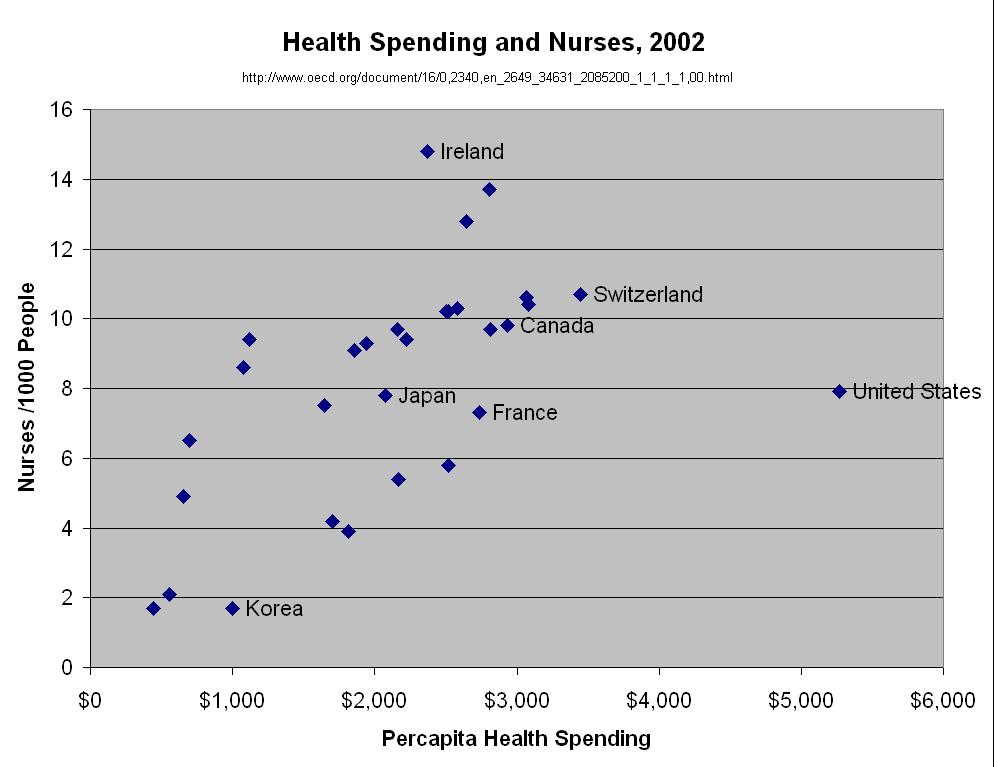
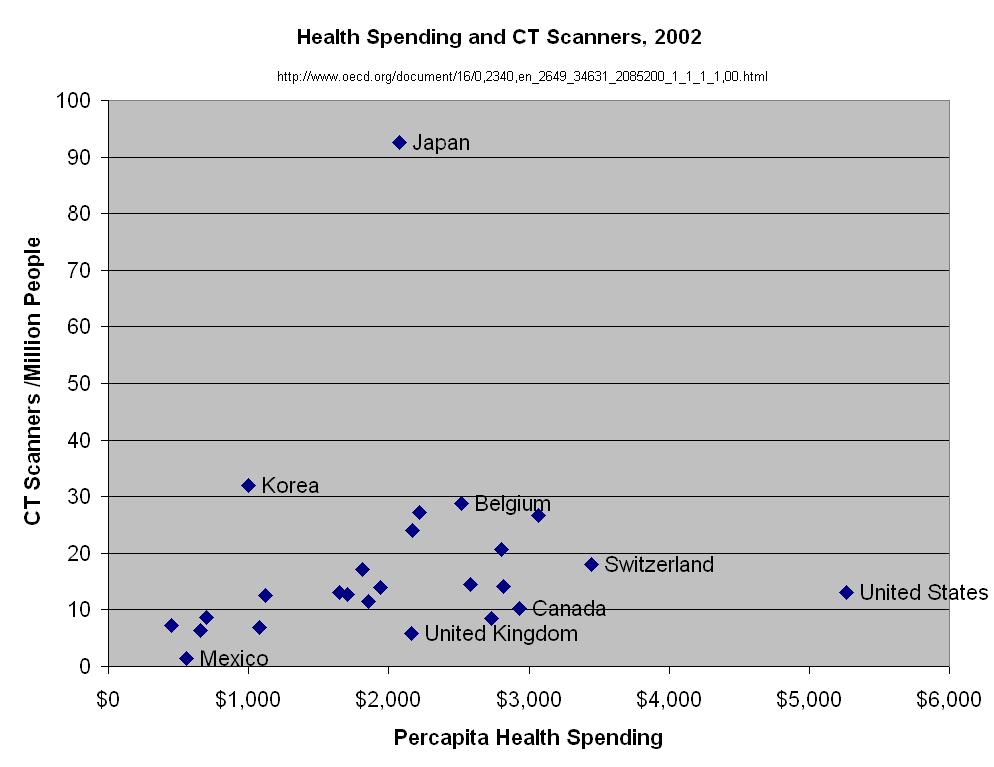
Health
Spending in the United States and the Rest of the Industrialized World,
by Gerard F. Anderson, Peter S. Hussey, Bianca K. Frogner, and Hugh R.
Waters, Health Affairs, 2005, Vol 24, Issue 4, 903-914. A USC campus computer may be required to
download this.This article shows how much more the U.S. spends on health care than other
countries. The article debunks some myths that are dear to the anti-reform crowd, particularly (1) that people in other
countries wait longer and get less service than Americans do, and (2) that
big malpractice tort awards are why U.S. health care costs so much.
"T.R. Reid: Looking Overseas For 'Healing Of America'". Well worth listening to. Reid's book, The Healing of America: A Global Quest for Better, Cheaper, and Fairer Health Care gives even more insight into health care system alternatives around the world, and is fun to read.
Paul Krugman gives the 700-word version in
"The Swiss Menace,"New York Times, August 16, 2009.
November 21
Pharmaceuticals
Learning objectives: Pharmaceutical prices, research, and sales
promotion. The dilemma of how to finance and promote
technological advance.
National Institute for Health Care Management Research and
Educational Foundation, Prescription Drugs and Intellectual
Property Protection Finding the Right Balance Between Access and
Innovation, July 24, 2000. Available at: http://www.nihcm.org/pdf/prescription.pdfRead quickly for the main idea, which is
illustrated in Figure 1.
Pharmaceuticals'
political contributionsBefore you glance at
this, guess which party gets the most from the drug industry. You can
also get the contributions breakdown for others industries and groups.
Check out nurses' contributions.
A 2005
British Medical Journal articleargued that countries
(like Britain) that negotiate lower drug prices are not free riders
benefitting from U.S.-consumer-financed industry research without
paying for it. Advanced countries that control drug prices create just as many new drugs, relative to the sizes of their economies, as the U.S does.
Pfizer and Abbott Labs earned all of their 2010 profit outside the U.S., according to Bruce Bartlett.
How American companies dodge taxes.
Blackboard Brennan, T.A., Sox, C.M., Burstin, H.R., "Relation Between
Negligent Adverse Events and the Outcomes of Medical-Malpractice
Litigation,"
N Engl J Med, December 26, 1996, 335(26), pp. 1963-1967. The skinny: There is not much relationship.
Blackboard Studdert, D.M., Mello, M.M., Gawande, A.A., Gandhi, T.K.,
Kachalia, A., Yoon, C., Puopolo, A.L., Brennan, T.A., "Claims, Errors,
and Compensation payments in Medical Malpractice Litigation," N
Engl J Med, May 11, 2006, Vol. 354, No. 18, pp. 2024-2033.
Public Citizen's Congress Watch, The 0.6 Percent Boogeyman, July 1, 2009. Medical malpractice tort costs have been falling (inflation-adjusted), and are down to 6/1000th of national health spending.
Quality without Insurance?
Rosen H, Fady Saleh F, Lipsitz S, Rogers SO, Gawande AA, Downwardly Mobile
The Accidental Cost of Being Uninsured, Arch Surg. 2009;144(11):1006-1011. Students have asked about the Emergency Medical Treatment and Active
Labor Act.
Socialized Medicine! In America!
Arnst, C., "The
Best Medical Care In The U.S., How Veterans Affairs transformed itself
-- and what it means for the rest of us," Business Week,
July 16, 2006. To find this article, go to www.businessweek.com and
type "Arnst" in the search box. Order the search by Newest first, then go to page 13.
Atul Gawande, "The Hot Spotters," The New Yorker, January 24, 2011. Another Gawande gem. A few patients incur much of health care cost. Well-organized primary care can achieve big savings.
Elliott S. Fisher, Douglas O. Staiger, Julie P.W. Bynum and Daniel J. Gottlieb, "Creating Accountable Care Organizations: The Extended Hospital Medical Staff," Health Affairs, 26, no. 1 (2007): w44-w57 online. The original idea
More medical practices are owned by hospitals than by doctors, according to one survey. I'll show the diagrams in class, so don't worry if you can't access this.
Blackboard Fisher ES et al, A Framework For Evaluating The Formation, Implementation, And Performance Of Accountable Care Organizations,
Health Aff November 2012 31:2368-2378. These first two are from the Dartmouth group that invented the ACO concept.
Blackboard Larson BK et al, Insights From Transformations Under Way At Four Brookings-Dartmouth Accountable Care Organization Pilot Sites,
Health Aff November 2012 31:2395-2406.
Blackboard Burns LR, Pauly MV, ANALYSIS & COMMENTARY: Accountable Care Organizations May Have Difficulty Avoiding The Failures Of Integrated Delivery Networks Of The 1990s,
Health Aff November 2012 31:2407-2416.
Atul Gawande again!, Big Med, The New Yorker, August 13, 2012. Managing health care as a production system, like a Chesscake Factory restaurant. Applied to to replacement knees.
Dec. 12 All assignments due by the end of this day.
The views and opinions expressed in this page are strictly those of the
page author. The contents of this page have not been reviewed or
approved by the University of South Carolina.
E-mail:
2013 stuff above. 2012 stuff below.
Supplemental articles (Read them if you're interested):
Blackboard
Goodman, J. C.,
Villarreal, P.,
and Jones, B.
"The Social Cost Of Adverse Medical Events, And What We Can Do About It"
Health Affairs April 2011 30:590-595; doi:10.1377/hlthaff.2010.1256

{kind=link}
{kind=link}
{kind=link}
{kind=link}