Last modified Monday, 26th October, 2020, 10:04am.
Too late for 2012's class, but Uwe Reinhardt has a succinct explanation of different insurance payment methods in his New York Times Economix blog post for December 7, 2012.
Professor Emeritus
Department of Health Services Policy and Management
Arnold School of Public Health
University of South Carolina
Columbia, SC 29208
E-mail:
Please put 712 in the
subject line
of course-related e-mail. Please see below for how to use Blackboard to submit course work.
The class meets at 3:30pm-5:50pm on Tuesdays in
Wardlaw 116. Map.
Class meetings are available live over the internet to registered students. The class meetings are recorded as well. Students can view the recordings at their convenience.
Office hours: Tuesdays 1pm to 3pm in the HSPM computer lab.
Goals
HSPM J712 introduces the application of economics to decisions
regarding the amount, organization, and distribution of health care
services in the United States. The goals of the course are:
to provide an economics perspective for management
decision-making
to provide theoretical groundwork for the study of finance,
accounting, marketing, and planning
to enable you as future health care managers to anticipate policy changes and their effects
to enable you as future health care managers to play positive
roles in the reform of health care
Competencies
You will demonstrate on the course's written assignments and through
class participation:
that you understand and can use basic economics concepts, such
as supply, demand, marginal analysis, the theory of capital, and
cost-benefit analysis,
that you can analyze the economic institutions of the United
States health care system,
that you can discuss controversies surrounding the development
of health insurance and the government's role in providing, financing,
and regulating health services.
What you need to have to take
this course
Prerequisite courses: None. No prior study of economics is
required for this course.
Required computer access: Students must have access to a
computer with:
internet access
a web browser with Java enabled (see box → )
The Adobe
Reader for pdf files. Get the free version. When you download and
install it, you can uncheck all
optional browser toolbars, etc.
Computers meeting these requirements are available for student use in
the Department's BlueCross BlueShield and
Companion Technologies Computer Education Center, on the first floor of
the HESC building.
Interactive instruction: A group of
interactive instructional tutorials is at https://sambaker.com/econ/.
The interactive tutorials introduce basic economics concepts, and assume no economics background. Your work with the
interactive tutorials is not monitored or graded. These
tutorials
are integrated into the Class Schedule and Readings, as shown below.
All
of the interactive tutorials are available all semester, so you can use
or reuse them at any time.
Course Work for Credit
Weekly comment:
Each week when there is a class, starting with week 2, but excluding the week of the mid-term, submit a substantive, relevant, comment.
The comment should be equivalent to about one-half to one page of 12-point single-spaced
type. For prose, that's 250 to 500 words. For poetry, you can have fewer words.
Comments are due by the start of class. They can be about that
class's ideas, or about the preceding class's ideas.
All comments that are on time and use course concepts will get full "A" credit.
Doing all the comments on time will give you the equivalent of an A for one-third of your
course grade.
Comments that are late or do not bring in course concepts will
get less than full credit.
Good comments can be about:
A personal or work experience that relates to an idea in the
readings or the lecture.
Your thoughts about an idea in the readings or lecture that seems
particularly interesting,
insightful, or pernicious.
A comparison of two readings' ideas.
You learn new concepts by using them. That is the purpose of the
comments.
Take-home exams are due on these dates:
Mid-term:
Tue., Oct. 9
Final:
Tue., Dec. 6
Each exam counts for one-third of the grade.
The exams will be distributed via this web page or Blackboard.
Your course grade is one-third the comments, one-third the mid-term
exam, and one-third the final exam.
Class Schedule and Readings
Advice for the overwhelmed: If the reading for this course seems
like a lot, see How
2 Read an Article.
August 28 Introduction to the Course -- no comment due
How the course will
operate, and the general shape of the US health care economic sector.
Stocks
and flowsDry, but helps with the next one. It also helps with understanding monetary policy, such as why the Federal Reserve can push a lot of money out to banks ("print money") during a recession and not spark price inflation.
The Gross Domestic ProductGo through for a general discussion of how this
important economic statistic is conceived.
U.S. National Health Spending in 2010:
Lecture notesI talk you through the most recent numbers for the size and shape of the
U.S. health care system.
For Blackboard readings, go to Blackboard, click the HSPMJ712 link, click on Content in the left menu, and then hunt through the Blackboard Readings list.
Blackboard Reinhardt, U.E., "Perspective: Spending More Through 'Cost
Control': Our Obsessive Quest to Gut the Hospital," Health
Affairs, Summer
1996, 15(2), pp. 145-154. A worthwhile
article. You see how a top-notch economist thinks. Relevant for this
week is how the author uses the "incremental cost" (marginal cost)
concept.
September 11
Cost-Benefit, Cost-Effectiveness, and
Cost-Savings Analysis comment
due
Methodology and ethics in cost-benefit
and
cost-effectiveness analysis, with application to evaluating the
cost-effectiveness of preventive care, the distinction between
cost-effective and cost-saving, and an attempt at policy based on
cost-effectiveness analysis.
Blackboard Axnick, N.W., Shavell, S.M., Witte, J.J., "Benefits Due to
Immunization Against Measles," Public Health Reports, August
1969, 84(8), pp. 673-680.
The
Colbert Report, July 14, 2008, on the declining value of life in the U.S. in the 2000s. U.S. government agencies and courts use a "hedonic" life value, rather than Axnick's basing a life value on the present value of expected future earnings. A hedonic life value is based on the difference between what dangerous jobs pay and what safer jobs pay. If you're curious, skim the 1976 article that originated the hedonic life value method.
Blackboard
Stack, M. L.,
Ozawa, S.,
Bishai, D. M.,
Mirelman, A.,
Tam, Y.,
Niessen, L.,
Walker, D. G.,
and Levine, O. S.
"Estimated Economic Benefits During The 'Decade Of Vaccines' Include Treatment Savings, Gains In Labor Productivity,"
Health Affairs June 2011 30:1021-1028
Blackboard
Goodman, J. C.,
Villarreal, P.,
and Jones, B.
"The Social Cost Of Adverse Medical Events, And What We Can Do About It"
Health Affairs April 2011 30:590-595; doi:10.1377/hlthaff.2010.1256
Blackboard
Van Den Bos, J.,
Rustagi, K.
Gray, T.,
Halford, M.,
Ziemkiewicz, E.,
and Shreve, J.
"The $17.1 Billion Problem: The Annual Cost Of Measurable Medical Errors,"
Health Affairs April 2011 30:596-603;
Blackboard Eddy, D.M., "Screening for Cervical Cancer," Annals of
Internal Medicine, August 1, 1990, 113(3), pp. 214-226. More technical. Don't get bogged down in technical detail.
See the notes for help with this.
Blackboard Fries, J.F., Koop, E., et al, "Reducing Health Care Costs by
Reducing the Need and Demand for Medical Services," N Engl J Med,
July 29, 1993, 329(5), pp. 321-325. The
authors are renowned public health leaders. This is conventional
wisdom. But is it right?
Blackboard Russell, L.B., "The Role of Prevention in Health Care Reform," N
Engl J Med, July 29, 1993, 329(5), pp. 352-354. Worth
a fairly careful read. What is the basis of Russell's disagreement with
the conventional wisdom?
Blackboard Huntington, J., Connell, F.A., "For Every Dollar Spent -- The
Cost-Savings Argument for Prenatal Care," N Engl J Med, Nov.
10, 1994, 331(19), pp. 1303-1307. Also
questions conventional wisdom.
Blackboard Eddy, D.M., Oregon's Methods: Did Cost-effectiveness Analysis
Fail?. JAMA, Oct. 16, 1991, 266(15), pp. 2135-2141. Uses the quality-adjusted life year. Oregon tried using cost-effectiveness analysis to decide which procedures Medicaid should pay for.
Supplemental:
The cost-effectiveness
of HPV vaccine. The study gives results with and without the discounting of
benefits that Eddy does in his PAP test study. Cost-effectiveness is
judged by dollars saved per quality-adjusted year of life saved. That
compares the vaccine with all efforts to save lives, rather than
comparing the vaccine just with other methods to control cervical cancer.
Prevention can save lives, and this one may save money, too: Finland reduced deaths from strokes and heart attacks by 75%, by working with the food industry to reduce salt. If that also meant fewer strokes, angina, and infarctions requiring surgery,
health care spending would be less, too. The New England Journal of Medicine, Sept. 1. 2009, had an article about hypertension in the U.S., where salt intake per person has increased 50% in the past 30 years.
Donna Richter, Prevention Key to Health Care Reform, The State, August 29, 2009. During 2009's health care reform battle, a version of the Fries-Koop argument from the 1993 health reform battle.
Arguments like that weren't just a distraction from the campaign to enact health insurance reform, they may have fed the paranoia about "death panels" that the opposition exploited. If you'd like a reminder of that craziness, here is Jon Stewart interviewing Betsy McCaughey (pronounced "McCoy") on the Daily Show August 20, 2009: Part 1 | Part 2.
September 18 No class meeting
Free Market concepts
-- comment due
What economists mean by markets, supply and demand, elasticity, and risk and risk aversion. These are building block concepts towards assessing having a free market in health care.
What things have to be true for the free market to give a good result. Are those things true for health care?
Health Care Demand -- How We Buy Health Care
Blackboard Bodenheimer, T., Grumbach, K., "Paying for Health Care," JAMA,
August 24/31, 1994, 272(8), pp. 634-639.
Information and uncertainty in health care choice, implications for letting the free market rule
Blackboard Arrow, K., "Uncertainty and the Welfare Economics of Medical
Care," American Economic Review, December 1963, 53(5),
pp. 941-973. Important. But difficult. Don't get bogged down. The blog posts below by Reinhardt will help, as will my notes below.
The trendy way to control health care spending is to have a big deductible and copayments. (Obamacare does exempt some "preventive" services.)
People do get less health care when
they have to pay more. To use the jargon, the demand for
health care has some elasticity. The elasticity is pretty low,
especially for people seeking care for serious symptoms, but it's not 0.
The articles go on to investigate whether people who buy less care are worse off as a result.
If they are not worse off, then it is wasteful to let people get care without paying out of pocket.
Are all the costs being considered? How good are people at determining what care they can do without?
Blackboard Brook, R.H., et al, "Does Free Care Improve Adults'
Health? Results from a Controlled Trial of Cost Sharing in Health
Insurance," N Engl J Med, December 8, 1983, 309, pp.
1426-1434.
Supplemental:Blackboard Himmelstein, D.U., Woolhandler, S., "Free Care, Cholestyramine,
and Health Policy," N Engl J Med, December 6, 1984, 311,
pp. 1511-1514.
Read quickly for the main ideas.
Blackboard Shapiro, M.F., Ware, J.F., Sherbourne, C.D., "Effects of Cost
Sharing on Seeking Care for Serious and Minor Symptoms," Annals of
Internal Medicine, February 1986, 104, pp. 246-251.
Read quickly for the main ideas.
Blackboard Rasell, M.E., "Cost Sharing in Health Insurance -- A
Reexamination," N Engl J Med, April 27, 1995, 332(17),
pp. 1164-1168.
Malcolm Gladwell, interviewed about "The Moral-Hazard Myth" on
the Al Franken Show (radio), August 25, 2005: A 19-minute mp3. The ideas in the article, with more implications drawn out. For those who like to hear, as well as read.
Gladwell said that the reason we don't have universal health insurance is that our leaders think that we're better off without it. Listen carefully to then-President Bush's "objective" for our health care system, from July 2007. It's in the first 20 seconds of the clip.
Blackboard Roe, B.B., "The UCR Boondoggle: A Death Knell for Private
Practice?" N Engl J Med, July 2, 1981, 305(1), pp.
41-45. Before Medicare introduced DRG-based payment, in 1983, fee-for-service was how most doctors and hospitals got paid.
Providers charged for each service rendered, setting prices according to what they thought they could or should get.
By the 1980s, prices had gotten seriously out of whack with costs.
Blackboard Reinhardt, U.E., "Resource Allocation in Health Care: The
Allocation of Lifestyles to Providers," The Milbank Quarterly,
1987, 65(2), pp. 153-176.
The allocation of resources was also out of whack.
Blackboard Brown, M.L., Kessler, L.G., Reuter, F.G., "Is the Supply of
Mammography Machines Outstripping Need and Demand?" Annals of
Internal Medicine, October, 1, 1990, 113(7), pp. 547-552. Excess
capacity did not lead to falling prices.
Blackboard Pattison, R.V., and Katz, H.M., "Investor-Owned and
Not-for-Profit Hospitals: A Comparison Based on California Data," N
Engl J Med, August 11, 1983, 309, pp. 347-353. More differences with the competitive model: Some
providers (for-profit hospitals, in this case) can charge more than
other providers for the same services.
DRG and RBRVS Lecture notesPricing in health care didn't follow the competitive market model, so the Federal government stepped in. Private insurers followed the government's lead.
Blackboard Simborg, D.W., "DRG Creep: A New Hospital-Acquired Disease," N
Engl J Med, June 25, 1981, 304(26), pp. 1602-1604.
Blackboard Baker, S.L., Kronenfeld, J.J., "Medicaid Prospective Payment:
Case-Mix Increase," Health Care Financing Review, Fall 1990, 12(1),
pp. 63-70.
RBRVS payment for doctors -- A tool for controlling physician fees
Blackboard Hsiao, W.C., Braun, P., Dunn, D., Becker, E.R., DeNicola, M.,
Ketcham, T.R., "Results and Policy Implications of the Resource-Based
Relative-Value Study," N Engl J Med, September 29, 1988, 319(13),
pp. 881-888.
Blackboard Hsiao, W.C., Braun, P., Yntema, D., Becker, E.R., "Estimating
Physicians' Work for a Resource-Based Relative Value Scale," N Engl
J Med, September 29, 1988, 319(13), pp. 835-841.
Where we are with pricing
Blackboard Reinhardt, Uwe E., "The
Pricing Of U.S. Hospital Services: Chaos Behind A Veil
Of Secrecy," Health Affairs,
January/February 2006; 25(1): 57-69.
Medical practice variation -- how much there is and why this matters.
If you have time for only one article, read the last one, by Gawande.
Blackboard Wennberg, J.E., McPherson, K., Caper, P., "Will Payment Based on
Diagnosis-Related Groups Control Hospital Costs?" N Engl J Med,
August 2, 1984, 311, pp. 295-300. People
living in different areas get very different care. This article created
a whole area of health services research.
Blackboard Hillman, B.J., Joseph, C.A., Mabry, M.R., Sunshine, J.H.,
Kennedy, S.D., Noether, M., "Frequency and Costs of Diagnostic Imaging
in Office Practice -- A Comparison of Self-Referring and
Radiologist-Referring
Physicians," N Engl J Med, Dec. 6, 1990, 323(23), pp.
1604-1608. A notorious example of the abuse of supply-sensitive care (see the Dartmouth Atlas readings below for what "supply-sensitive care" is)
The Dartmouth Atlas, http://www.dartmouthatlas.org/, has extensive data
and analysis on medical practice variation. They argue that there are three categories of medical care. Here they are, with links to reports:
Effective care, which is clearly indicated for the diagnosis
Atul Gawande, The Cost Conundrum: What a Texas Town Can Teach Us about Health Care, The New Yorker, June 1, 2009. President Obama had all his policy people read this.
October 30
Market outcomes: Transactions (administrative) cost, in the U.S. and elsewhere. Comment due
Administrative cost in U.S. health care
Blackboard Himmelstein, D.U., Woolhandler, S., "Cost Without Benefit:
Administrative Waste in U.S. Health Care," N Engl J Med,
February 13, 1986, 314, pp. 441-445. Letters and authors'
rejoinder, N Engl J Med, October 16, 1986, 315, pp.
1033-1035.
Supplemental (but cute):Blackboard Grumet, G.W., "Health Care Rationing Through Inconvenience: The
Third Party's Secret Weapon," N Engl J Med, August 31, 1989, 321(9),
pp. 607-611.
Blackboard Woolhandler, S., Himmelstein, D.U., "The Deteriorating
Administrative Efficiency of the U.S. Health Care System," N Engl J
Med, May 2,
1991, 324(18), pp. 1253-1258.
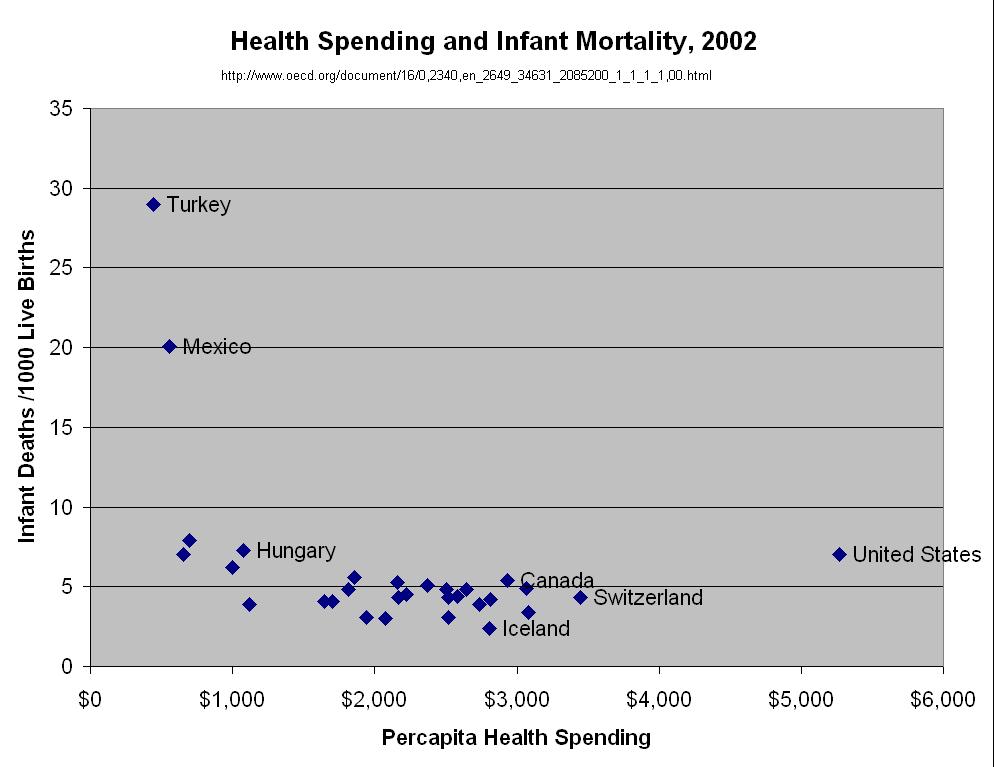
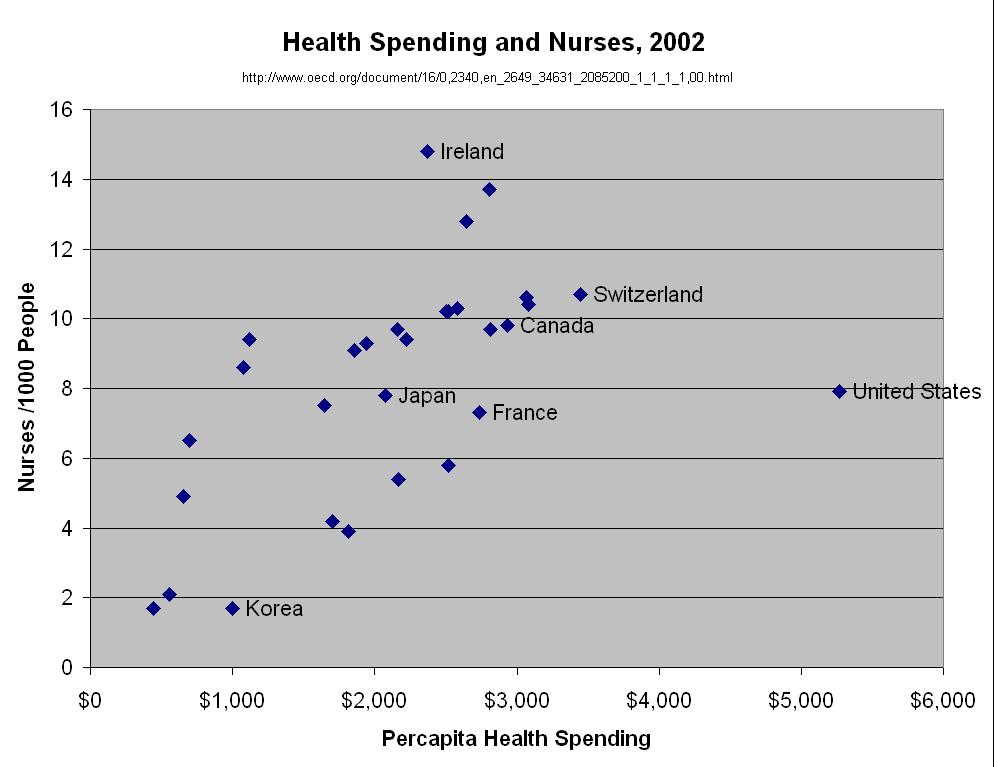
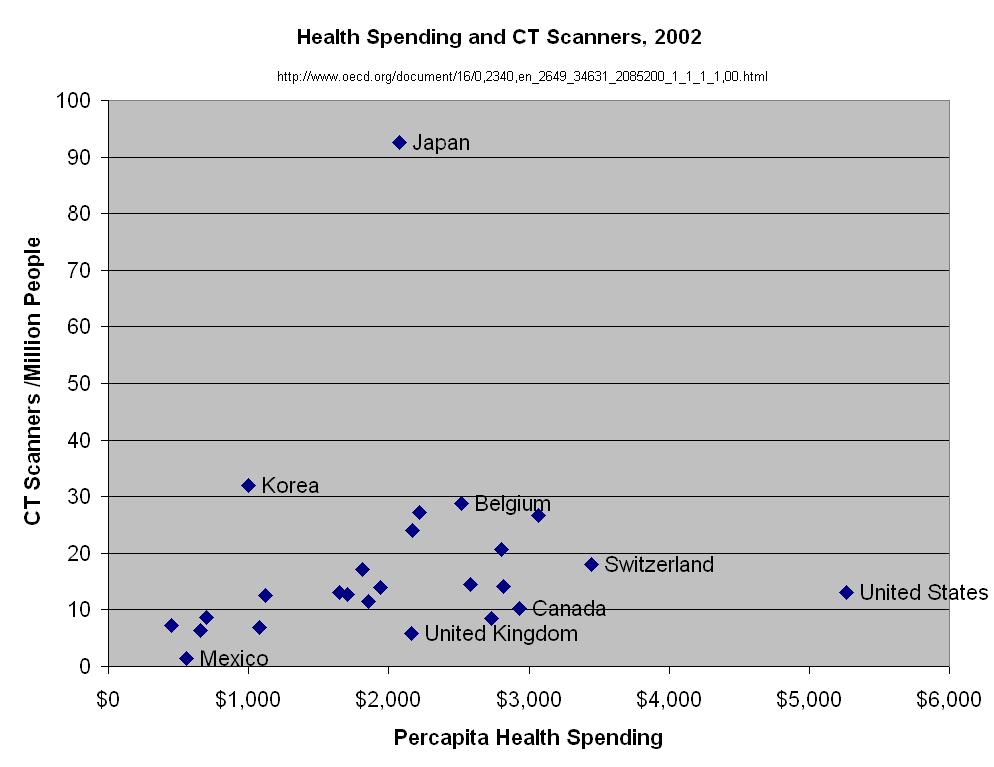
Health
Spending in the United States and the Rest of the Industrialized World,
by Gerard F. Anderson, Peter S. Hussey, Bianca K. Frogner, and Hugh R.
Waters, Health Affairs, 2005, Vol 24, Issue 4, 903-914. A USC campus computer may be required to
download this.This article shows how much more the U.S. spends on health care than other
countries. The article debunks some myths that are dear to the anti-reform crowd, particularly (1) that people in other
countries wait longer and get less service than Americans do, and (2) that
big malpractice tort awards are why U.S. health care costs so much.
"T.R. Reid: Looking Overseas For 'Healing Of America'". Well worth listening to. Reid's book, The Healing of America: A Global Quest for Better, Cheaper, and Fairer Health Care gives even more insight into health care system alternatives around the world, and is fun to read.
Paul Krugman gives the 700-word version in
"The Swiss Menace,"New York Times, August 16, 2009.
Learning objectives: The history and results managed care and private health insurance.
Managed care development
Blackboard Mayer, T.R., and Mayer, G.G., "HMOs: Origins and Development" N
Engl J Med, February 28, 1985, 312, pp. 590-594.
When HMOs were cool
BlackboardWare, J.E., et al, "Comparison of Health Outcomes at a Health
Maintenance Organisation with Those of Fee-for-Service Care," Lancet,
May 3, 1986, pp. 1017-1022.
Blackboard Siu, A.L., Leibowitz, L., Brook, R.H., Goldman, N.S., Lurie, N.,
Newhouse, J.P., "Use of the Hospital in a Randomized Trial of Prepaid
Care," JAMA, March 4, 1988, 259, pp. 1343-1346.
Supplemental:Blackboard Ware, J.E., Bayliss, M.S., Rogers, W.H., Kosinski, M., Tarlov
A.R., "Differences in 4-year Health Outcomes for Elderly and Poor,
Chronically Ill Patients Treated in HMO and Fee-for-Service
Systems: Results from the Medical Outcomes Study," JAMA,
October 2, 1996, 276(13), pp. 1039-1047.
Blackboard Bodenheimer, T.S., and Grumbach, K., "Capitation or
Decapitation," JAMA, October 2, 1996, 276(13), pp.
1025-1031. How the money flows in IPA HMOs
Blackboard Kuttner, R., "Must Good HMOs Go Bad? First of Two Parts: The
Commercialization of Prepaid Group Health Care," N Engl J Med
May 21, 1998, 338(21), pp. 1558-1563.
Blackboard Himmelstein, D.U., Woolhandler, S., Hellander, I., Wolfe, S.M.,
"Quality of Care in Investor-Owned vs Not-for-Profit HMOs," JAMA.
July 14, 1999, 282:159-163
Medicare HMOs
Blackboard Morgan, R.O., Virnig, B.A., DeVito, C.A., Persily, N.A., "The
Medicare-HMO Revolving Door -- The Healthy Go In and the Sick Go Out," N
Engl J Med, July 17, 1997, 337(3), pp. 169-175.
Blackboard Needleman, J., Buerhaus, P., Mattke, S., Stewart, M., Zelevinsky,
K., "Nurse-Staffing Levels and the Quality of Care in Hospitals," N
Engl J Med, May 30, 2002, 346(22), pp. 1715-1722. An example of quality variation that the market does not
solve. Read quickly for the main ideas.
November 20 Malpractice; Bankruptcy; The Uninsured comment due
Malpractice
Blackboard Brennan, T.A., Sox, C.M., Burstin, H.R., "Relation Between
Negligent Adverse Events and the Outcomes of Medical-Malpractice
Litigation,"
N Engl J Med, December 26, 1996, 335(26), pp. 1963-1967. The skinny: There is not much relationship.
Blackboard Studdert, D.M., Mello, M.M., Gawande, A.A., Gandhi, T.K.,
Kachalia, A., Yoon, C., Puopolo, A.L., Brennan, T.A., "Claims, Errors,
and Compensation payments in Medical Malpractice Litigation," N
Engl J Med, May 11, 2006, Vol. 354, No. 18, pp. 2024-2033.
Supplemental:Blackboard Jena, A. B., Seabury, S., Lakdawalla, D., Chandra, A., "Malpractice Risk According to Physician Specialty," N Engl J Med 2011; 365:629-636 August 18, 2011.
Public Citizen's Congress Watch, The 0.6 Percent Boogeyman, July 1, 2009. Medical malpractice tort costs have been falling (inflation-adjusted), and are down to 6/1000th of national health spending.
Supplemental: A Wal-Mart executive's memo
proposing that they "dissuade unhealthy people from coming to work at
Wal-Mart" by increasing health insurance copayments and making all jobs
physically demanding, Nov. 2005.
In 2006, people paid for health insurance, then Blue Cross (of California) revoked it when they got
sick. This illustrates, in an extreme way, the lack of consumer
sovereignty in the health insurance market, which compounds the problem
of lack of consumer sovereignty in health care markets. Here are the stories, from the L.A. Times.
Rosen H, Fady Saleh F, Lipsitz S, Rogers SO, Gawande AA, Downwardly Mobile
The Accidental Cost of Being Uninsured, Arch Surg. 2009;144(11):1006-1011. Students have asked about the Emergency Medical Treatment and Active
Labor Act.
November 27 Obamacare and health care reform
comment
due
Supplemental: Newhouse, Joseph P., "Assessing Health Reform's Impact
on Four Key Groups of Americans, Health Affairs 29:9, September 2010, pp. 1714-1725.
Arnst, C., "The
Best Medical Care In The U.S., How Veterans Affairs transformed itself
-- and what it means for the rest of us," Business Week,
July 16, 2006. To find this article, go to www.businessweek.com and
type "The Best Medical Care In The U.S." in the search box. Then look down the list for this July 2006 article. (I found it on the second page. To read the article, I had to login to Facebook. Will all my Friends get ads from Bloomberg Business Week?)
Accountable Care Organizations and Primary Care Reform
Atul Gawande, "The Hot Spotters," The New Yorker, January 24, 2011. Another Gawande gem. A few patients incur much of health care cost. Well-organized primary care can achieve big savings.
Elliott S. Fisher, Douglas O. Staiger, Julie P.W. Bynum and Daniel J. Gottlieb, "Creating Accountable Care Organizations: The Extended Hospital Medical Staff," Health Affairs, 26, no. 1 (2007): w44-w57 online. The original idea
More medical practices are owned by hospitals than by doctors, according to one survey. I'll show the diagrams in class, so don't worry if you can't access this.
National Institute for Health Care Management Research and
Educational Foundation, Prescription Drugs and Intellectual
Property Protection Finding the Right Balance Between Access and
Innovation, July 24, 2000. Available at: http://www.nihcm.org/pdf/prescription.pdfRead quickly for the main idea, which is
illustrated in Figure 1.
Pharmaceuticals'
political contributionsBefore you glance at
this, guess which party gets the most from the drug industry. You can
also get the contributions breakdown for others industries and groups.
Check out nurses' contributions.
Behind a pay wall, sorry! The skinny: Developed countries develop new drugs in proportion to how big their economies are. If drug price controls curtailed innovation then the US would produce proportionally more new drugs, but we don't.A
British Medical Journal article argues that countries
(like Britain) that negotiate lower drug prices are not free riders
benefitting from U.S.-consumer-financed industry research without
paying for it.
Pfizer and Abbott Labs earned all of their 2010 profit outside the U.S., according to Bruce Bartlett.
The views and opinions expressed in this page are strictly those of the
page author. The contents of this page have not been reviewed or
approved by the University of South Carolina.
E-mail:

{kind=link}
{kind=link}
{kind=link}
{kind=link}